


Blood Pressure Monitor: Design, Manufacturing, and Future Trends
Background
Blood pressure is the force exerted by circulating blood against the walls of arteries. The pulse, a rhythmic surge of blood from the left ventricle into the aorta, drives this pressure wave through the circulatory system. Clinicians assess two key points of the wave using a sphygmomanometer (blood pressure monitor): the systolic pressure, the peak value during ventricular contraction, and the diastolic pressure, the lowest value when the heart relaxes. These measurements, expressed in millimeters of mercury (mmHg), are critical for evaluating cardiovascular health and diagnosing disease.
A traditional cuff‑based sphygmomanometer is paired with a stethoscope. After wrapping the cuff around the upper arm, the clinician inflates it with a rubber bulb until the pressure indicator—often a mercury column or aneroid dial—stops moving, typically between 150 and 200 mmHg. The stethoscope is placed over the brachial artery; as the cuff slowly deflates, the first audible Korotkoff sound marks systolic pressure, and the disappearance of sound marks diastolic pressure. Normal ranges are approximately 110–140 mmHg systolic and 65–80 mmHg diastolic. Elevated readings raise the risk of heart disease, stroke, and kidney failure.
Early attempts at direct arterial measurement were invasive and hazardous. The first cuff‑based device was introduced by Samuel Siegfried von Basch in 1876. Two decades later, Scipione Riva‑Rocci refined the design, enabling more accurate readings. In 1905, Nikolai Korotkoff added the stethoscope, allowing measurement of both systolic and diastolic pressures. Today, both values are essential for comprehensive cardiovascular assessment.
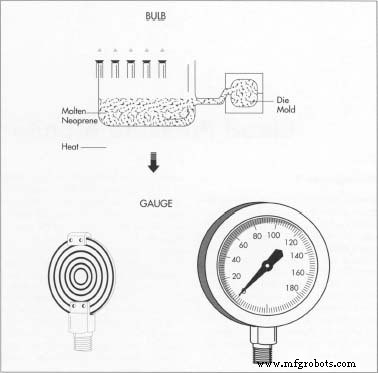
The neoprene bulb is typically formed via vacuum‑assisted injection molding. Molten neoprene is injected into a two‑piece metal die while a vacuum draws out air through tiny holes, ensuring even wall thickness. After cooling, the bulb is trimmed and ready for assembly. The pressure gauge may feature a mercury manometer or an electronic display; most still use a durable aneroid dial for its reliability and low cost.
Design
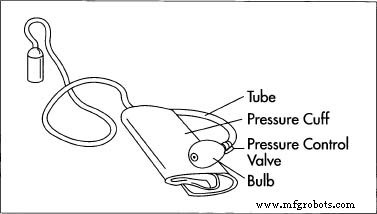
All blood pressure monitors share core components: a pump bulb, a control valve, a pressure indicator, a cuff, and connecting hoses. Three primary designs exist: (1) mechanical gauge, (2) mercury manometer, and (3) electronic display. While digital models are gaining traction, gauge‑type monitors remain popular for their ease of service, accuracy, durability, and affordability. This article focuses on the aneroid gauge variant.
The standard system includes a neoprene or rubber bulb, a valve with a one‑way flow mechanism, and a cuff consisting of a fabric‑lined neoprene bladder with Velcro fastener. Hoses made by continuous extrusion link the bulb to the cuff and gauge. The valve’s internal rubber disk seals the bulb during inflation and opens during deflation, ensuring precise pressure control.
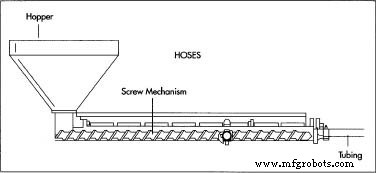
Rubber hoses are produced by extruding molten rubber through a die that shapes the tubing around a central rod, then cooling, cutting, and coiling them for shipment to the assembly line.
Raw Materials
The aneroid gauge comprises a pressure element (two phosphor‑bronze disks), a movement assembly (polycarbonate or brass gear train), and a protective case with a viewing lens. The pointer is aluminum, while the dial may be brass, aluminum, or plastic. The squeeze bulb and hoses are made of rubber or neoprene; the cuff’s bladder is fabric‑lined neoprene, and the valve may be polycarbonate, brass, stainless steel, or composite. Each material is selected for durability, flexibility, and biocompatibility.
The Manufacturing Process
Manufacturers often source components separately, then assemble and package the final unit. Each part follows a dedicated production workflow:
The Bulb
- Bulbs are most commonly fabricated via vacuum‑assisted injection molding. Molten rubber is forced into a metal die; a vacuum draws out air through fine perforations, promoting uniform wall thickness. The material solidifies within seconds, then the bulb is trimmed and inspected.
The Valves
- Valves are produced by die casting, plastic injection molding, or machining from bar stock. Precision CNC machining shapes threads and internal features, ensuring reliable coupling with the bulb and hoses.
While gauge‑based monitors will continue to thrive for their portability, electronic displays are expected to rise with advances in power supply and rugged design. Mercury‑based units are likely to decline due to environmental concerns.
The Gauge
- The gauge contains a pressure element formed by soldering two phosphor‑bronze disks into a hollow wafer. Pressure from the cuff causes the wafer to swell, moving a gear train that turns the pointer. Calibration involves connecting the gauge to a master pressure source and fine‑tuning the movement linkage until readings match the reference.
The Cuff
- The cuff bladder is created by heat‑sealing two rubber sheets, integrating a tubing fitting for air supply, then covering it with fabric for comfort and durability.
The Hoses
- Hoses are extruded from rubber pellets heated to a viscous state, forced through a die with a central rod. As the material cools, it forms the desired tubing, which is then cut, spooled, and shipped.
Assembly
- During final assembly, hoses connect all components. Leak tests and calibration checks confirm performance. The process exemplifies just‑in‑time (JIT) procurement and total quality control (TQC), ensuring each part meets stringent standards before final product release.
The Future
Manufacturers face increasing liability exposure for product failures. Mercury instruments are being phased out due to hazardous material concerns, while electronic models are poised to grow as power solutions improve. Regardless of technological shifts, accurate blood pressure measurement remains indispensable for clinical practice, ensuring that sphygmomanometers—whether gauge, mercury, or digital—will continue to play a vital role in patient care.
Manufacturing process
- Insulin: Biology, Production, and Emerging Therapies
- Artificial Heart: Technology, History, and Future Prospects
- Artificial Blood: Current Status, Development, and Future Prospects
- Fire Extinguishers: Types, Design, and Future Trends
- Precision Pressure Gauges for Industrial & Safety Applications
- Blood Pressure Sensor: How It Works & Key Applications
- Advanced Home Monitoring System with Arduino Mega and IoT Sensors
- Advanced Arduino-Based ECG Monitor for Real-Time Heart Rate Detection
- Soft Neck Patch: First All‑in‑One Wearable for Continuous Blood Pressure, Heart Rate, and Biochemical Monitoring
- UC San Diego's Smart Skin Patch Offers Real-Time Blood Pressure, Heart Rate, and Biochemical Monitoring