


Artificial Eye Prostheses: From History to Cutting‑Edge Innovation
Background
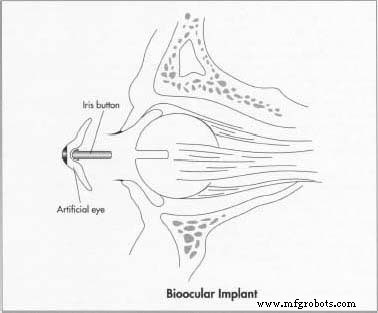
An artificial eye is a cosmetic prosthesis that replaces a natural eye lost to injury or disease. While it does not restore vision, it occupies the eye socket, improves facial symmetry, and, when attached to the socket’s muscles, can mimic natural eye movement.
Modern artificial eyes are predominantly made of durable plastic and typically last around ten years. Children, however, often need more frequent replacements because their sockets grow as they mature—four to five prostheses may be required from infancy to adulthood.
According to the Society for the Prevention of Blindness, 10,000 to 12,000 people in the U.S. lose an eye each year. Over 50% of these losses are injury‑related, with a higher incidence in males. Genetic conditions such as microphthalmia, anophthalmia, retinoblastoma, cataracts, and glaucoma also contribute to ocular loss, with 63% of disease‑related cases occurring before age 50.
Two surgical approaches are used to remove a damaged eye. Enucleation removes the entire globe and associated muscles, after which an orbital implant restores volume and allows artificial eye movement. Evisceration removes only the eye’s contents, leaving the scleral shell intact; an inert material ball is inserted before closure. A conformer—a silicone or hard‑plastic disc—is placed immediately post‑op to prevent socket shrinkage and preserve the pocket for the prosthesis. Healing typically takes four to six weeks, after which a skilled ocularist customizes the artificial eye.
History
Early prostheses were more decorative than functional, crafted by artisans in ancient Babylon, Jericho, Egypt, China, and the Aegean for religious or aesthetic purposes. Excavations reveal silver, gold, crystal, and glass eyes in mummies and tombs, indicating a long tradition of ocular craftsmanship.
In 1579, Venetian surgeons introduced the first eyelid‑mounted glass shell, which, despite its thinness, failed to restore socket volume and caused discomfort, necessitating nightly removal.
The 19th century saw significant progress. German glassblower Ludwig Müller‑Uri refined a life‑like glass eye for his son, eventually establishing a full‑time business. Dutch ophthalmologist Hermann Snellen’s 1880 “Reform” design added thickness and rounded edges, improving comfort and volume restoration. Germany quickly became the hub for glass prosthesis manufacturing.
1884 marked the first scleral‑cavity implantation of a glass sphere by English doctor Phillip Henry Mules, a technique that later extended to enucleated sockets. Over a century later, the Mules sphere remains the standard for many evisceration cases.
During World War II, German glass supplies were cut off, prompting U.S. Army dental technicians to create the first plastic prosthesis in 1943—unbreakable but with a rough back surface that irritated the socket. Subsequent adaptations by German‑American glassblowers improved fit and comfort, yet persistent mucus discharge and the need for daily cleaning remained challenges. Large optical firms began mass‑producing standardized “stock” glass shapes, though these lacked individualized fit.
The late 1960s introduced Lee Allen’s modified impression technique, which accurately captured the socket’s contour and allowed precise front‑surface customization, setting the standard still used today.
Raw Materials
Plastic forms the core of modern artificial eyes. Wax and plaster of Paris create molds; alginate, a seaweed‑derived powder, captures the socket’s exact shape. Artists apply specialized paints and dyes to render realistic irises and scleral tones.
Manufacturing Process
The time from initial consultation to finished prosthesis averages 3½ hours, though timelines vary by ocularist and patient complexity. Two primary prosthesis types exist: thin shell eyes for partially missing or disfigured sockets, and fully modified impression prostheses for complete eye removal.
- Inspect the socket, measuring horizontal, vertical dimensions, and peripheral contour.
- Paint a custom iris on a plastic button; typical diameters range from 0.4–0.52 in (10–13 mm). The button’s color is matched by viewing it through the prosthetic dome.
- Carve a wax shell embedding the iris button, then fit it to the socket, adjusting as needed until the button aligns with the remaining eye. Two relief holes are then drilled.
- Apply alginate to the wax shell’s backside, insert into the socket, and allow it to set for ~2 minutes, capturing an accurate impression. Remove the shell, leaving the alginate impression attached to the wax.
- Re‑verify iris color and reinsert the conformer.
- Cast a plaster‑of‑paris model from the impression. Once hardened (~7 min), discard the wax and alginate, and embed the painted iris into the plaster.
- Pour molten white plastic into the mold, re‑assemble the halves, and cure under pressure in boiling water (~23 min). Cool, then trim 0.5 mm from the anterior surface to simulate scleral overlap.
- Apply scleral pigments using paint, chalk, or thread; adjust iris color as needed. Insert clear plastic into the anterior half, re‑press, and cure (~30 min). Finish with grinding and polishing to achieve a high luster, essential for comfort.
Quality Control
The American Society of Ocularists (ASO), founded in 1957, raised industry standards and introduced certification in 1971. The National Examining Board for Ocularists (NEBO), established by NCHCA in 1980, administers a national exam; board‑certified ocularists must recertify every three years. Fellowship requires 375 additional credit hours and demonstrable expertise.
The Future
Innovations continue to enhance both comfort and functionality. Early 1980s saw the first interchangeable‑pupil prosthesis, followed by a soft contact lens with a large black pupil for easy placement. In 1989, the FDA approved the BioEye—an implant made of hydroxyapatite, a coral‑derived ceramic that mimics bone’s porous structure, reducing migration and improving eyelid support.
Advances in microelectronics and image‑processing promise artificial eyes that could restore vision. Canadian researchers are developing a prosthesis that interfaces directly with the optic nerve or visual cortex, featuring a rubbery lens, high‑precision color processor, and micro‑photoreceptors. Parallel efforts at MIT and Harvard aim to create an artificial retina using a biochip that glues to ganglion cells, translating infrared laser signals into visual data via a sensor system worn on the wearer’s glasses.
While a fully functional sight‑restoring prosthesis remains years away, the trajectory of research offers hope for unprecedented restoration of both appearance and vision.
Manufacturing process
- Artificial Turf: From AstroTurf to Modern Hybrid Surfaces
- Artificial Heart: Technology, History, and Future Prospects
- Artificial Heart Valves: Types, History, and Future Innovations
- Artificial Blood: Current Status, Development, and Future Prospects
- The Evolution and Craftsmanship of Artificial Flowers: From Silk to Modern Perma‑Stem
- How Artificial Snow Machines Transform Winter Sports
- Artificial Skin: Advanced Tissue Engineering for Burns, Wounds, and Future Regenerative Therapies
- The Evolution and Modern Science of Prosthetic Limbs
- Artificial Intelligence in Retail: Proven Benefits, Not a Fad
- Big Data vs AI: Synergy Behind Digital Transformation