


The Evolution and Modern Science of Prosthetic Limbs
Background
Artificial arms and legs, known as prostheses, are engineered to restore functional capabilities to individuals who have undergone amputation. Mechanical assistive devices enabling ambulation or dual‑hand use date back to antiquity, with the simple peg leg being the most recognizable early example. Successful surgical amputation techniques only emerged around 600 B.C., after which medieval armorers fabricated early prosthetic limbs from rigid iron. Despite incorporating articulated joints introduced by Ambroise Paré in the 1500s, these early devices offered limited voluntary control. Subsequent advancements in the 18th and 19th centuries—such as Peter Baliff’s below‑elbow design (1812) and Van Peetersen’s above‑elbow model (1844)—improved functionality, yet still fell short of modern standards.
The nineteenth century marked a pivotal shift driven by amputees themselves. Civil War engineer J.E. Hanger lost a leg, designed a custom prosthetic, and founded the enduring J.E. Hanger Company in 1861. Likewise, A.A. Winkley developed a slip‑socket below‑knee device and, with Lowell Jepson, launched the Winkley Company in 1888. Their products were showcased at the National Civil War Veterans Reunion, cementing their commercial presence.
D.W. Dorrance, who lost his right arm in an accident, introduced a terminal hook in 1909 that significantly improved grasping ability. Prior to his invention, prosthetic arms relied on leather sockets, heavy steel frames, and passive hooks or rudimentary mechanical hands. Dorrance’s split hook—anchored to the contralateral shoulder and actuated by a strap and rubber bands—restored functional prehension and remains a cornerstone of modern hook designs, often concealed beneath realistic skin.
The twentieth century witnessed transformative progress as new materials such as plastics replaced iron and wood, resulting in lighter, stronger, and more cosmetically appealing devices. A watershed innovation was the advent of myoelectric prostheses in the late 1940s, enabling limb movement through the patient’s own muscle‑generated electrical signals. By the 1960s myoelectric devices were available for adults, and the last decade has seen widespread adoption in pediatric care.
In recent years, computer‑aided design and manufacturing (CAD/CAM) have become standard in private prosthetic practices. Eighty‑five percent of clinics now employ CAD/CAM to model a patient’s arm or leg, producing precise molds for custom sockets. Techniques such as vacuum‑forming and laser‑guided measurement further refine fit and comfort.
Raw Materials
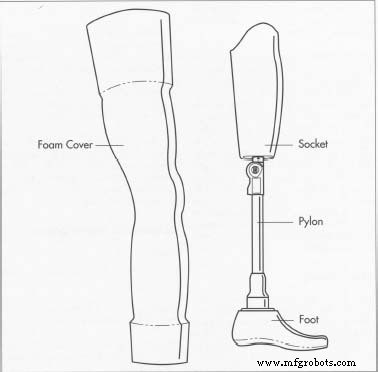
A typical prosthetic consists of a custom‑fitted socket, an internal structure (pylon), knee cuffs or belts, prosthetic socks, and, in some cases, realistic skin. Material selection prioritizes lightness and durability: polypropylene is common for sockets, while titanium and aluminum alloys replace steel in pylons. Recent innovations favor carbon fiber for its exceptional strength‑to‑weight ratio.
Feet historically used hardwoods—maple, hickory, basswood, willow, poplar, and linden—combined with rubber. Modern feet are usually urethane foam cores with wooden keels, supplemented by polyethylene, polypropylene, acrylics, and polyurethane for other components. Prosthetic socks are made from soft yet resilient fabrics, ranging from wool and cotton to advanced synthetics.
Visual aesthetics are critical. Most endoskeletal prostheses feature a polyurethane foam cover molded to match the contralateral limb, then overlaid with a custom‑painted artificial skin that replicates the patient’s natural hue.
The Manufacturing Process
Prosthetic limbs are not mass‑produced retail items; they are bespoke solutions. After a medical prescription—typically following a multidisciplinary evaluation—patients visit a prosthetist for fitting. While certain components (e.g., sockets) are custom fabricated, others such as feet and pylons are pre‑manufactured and assembled on site. A few advanced centers produce the entire limb in‑house.
Measuring and Casting
- 1. Accurate measurements are essential to create a comfortable, functional limb. The prosthetist first evaluates the residual limb, taking an impression or digital scan.
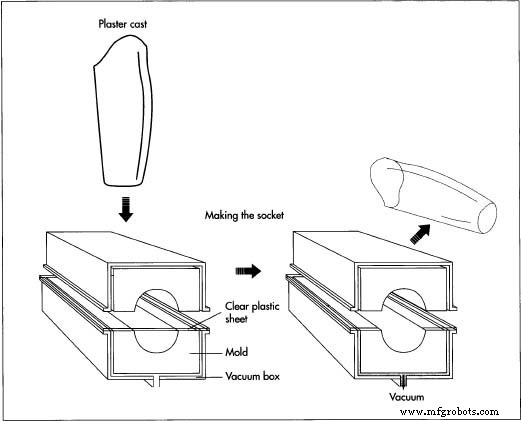
- 2. Using these data, the prosthetist records segment lengths and the positions of remaining bones and tendons. A plaster‑of‑Paris cast is then produced, capturing a detailed positive model of the stump.
Making the Socket
- 3. A clear thermoplastic sheet is heated in an oven and vacuum‑formed over the positive mold. This process yields a transparent test socket that allows the prosthetist to assess fit visually.
- 4. The test socket is fitted to the patient. For lower‑limb amputees, the patient walks while the prosthetist observes gait and comfort. Adjustments are made by reheating the thermoplastic; thicker socks can be added for cushioning.
- 5. Once finalized, the permanent socket—typically polypropylene—is vacuum‑formed in the same manner. Stumps may shrink after surgery, stabilizing after about a year; sockets are therefore often replaced at that time or when anatomical changes necessitate a new fit.
Fabrication of the Prosthesis
- 6. Components are manufactured using standard plastic processing methods: vacuum‑forming, injection molding, extrusion, die‑casting for metal pylons, and woodworking for wooden parts. Assembly uses bolts, adhesives, and laminates.
- 7. The technician assembles the limb, often with tools such as torque wrenches. The prosthetic device—shown in the image below—is then fitted to the patient. Final adjustments ensure optimal alignment and comfort.
Physical Therapy
Successful adaptation to a prosthetic limb requires comprehensive training. Patients must learn to manage the device, strengthen the residual musculature, and perform daily tasks. In myoelectric cases, muscle conditioning is particularly important to generate sufficient electrical signals. Regular cleaning and donning/doffing practice are also emphasized.
Individuals fitted with artificial arms learn to operate the limb, its locking mechanisms, and the terminal device. The learning curve differs between traumatic amputees—who may adapt quickly—and those with congenital absence, who may face greater challenges. Structured instruction systems enable single‑handed manipulation of everyday objects.
For leg amputees, physical therapy typically spans 18–20 weeks to regain ambulation. Patients also practice transferring between beds and cars, navigating inclines, and safe fall‑recovery techniques.
Quality Control
While the United States lacks a unified regulatory framework for prosthetic limbs, many manufacturers adopt European ISO standards, particularly when exporting to Europe. Critics argue these guidelines can be overly stringent; proponents maintain that harmonized standards ensure safety and performance.
Independent testing assesses mechanical strength and durability. Static load tests involve applying force over a 30‑second period, holding for 20 seconds, then releasing over 30 seconds, verifying no deformation. Failure tests push the limb to its breaking point to define strength limits. Cyclic load tests simulate long‑term use—two million cycles at one per second approximates five years of daily activity. Successful prototypes typically endure at least 250,000 cycles.
The Future
Experts envision a prosthetic limb that is both technologically sophisticated and user‑friendly. The ideal device would be intuitive, low‑maintenance, comfortable, lightweight, adaptable, natural‑looking, and easy to clean. Recent advances bring us closer to this goal.
Carbon fiber, celebrated for its high strength and lightness, is increasingly employed as the core material for endoskeletal pylons, potentially replacing metals entirely.
Innovative software overlays a pressure grid onto a patient’s CT scan, allowing the prosthetist to design sockets that minimize tissue compression and pain. Experimental pressure‑sensing feet transmit ground‑reaction data to electrodes embedded in the stump, enabling proprioceptive feedback and more natural gait patterns.
Moreover, programmable above‑knee prostheses incorporate onboard computers that adapt to the wearer’s gait, delivering smoother, more automatic walking dynamics.
Manufacturing process
- Artificial Turf: From AstroTurf to Modern Hybrid Surfaces
- Artificial Heart: Technology, History, and Future Prospects
- Artificial Heart Valves: Types, History, and Future Innovations
- Artificial Blood: Current Status, Development, and Future Prospects
- The Evolution and Craftsmanship of Artificial Flowers: From Silk to Modern Perma‑Stem
- How Artificial Snow Machines Transform Winter Sports
- Artificial Eye Prostheses: From History to Cutting‑Edge Innovation
- Artificial Skin: Advanced Tissue Engineering for Burns, Wounds, and Future Regenerative Therapies
- AI-Powered Obstacle Avoidance System with Arduino and Ultrasonic Sensors
- Bionic Sportsmen: Cutting-Edge Prosthetics Empowering Athletic Equality