


Stethoscope: History, Design, and Modern Manufacturing
Background
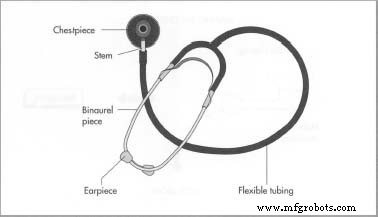
A stethoscope is a medical instrument that amplifies internal body sounds—especially those from the heart and lungs—to aid clinicians in diagnosis. Modern stethoscopes are binaural, featuring two flexible rubber tubes that connect a central valve to earplugs. The chestpiece at the tip can be either a bell‑shaped low‑frequency receiver or a flat diaphragm for higher frequencies. Clinicians use the device to detect heart murmurs, arrhythmias, and abnormal lung sounds such as wheezes or crackles.
The invention is credited to René‑Théophile‑Hyacinthe La Ne c, who in 1819 replaced the naked eye with a wooden cylinder—later called the “baton”—to amplify a patient’s heartbeat. La Ne c observed that sound is transmitted efficiently through wood, a principle he applied to create a hollow wooden tube approximately 15 cm long, shaped like a trumpet. The baton allowed physicians to hear faint cardiac sounds for the first time.
Early stethoscopes were monaural and made of wood (cedar or pine). They ranged from 15 cm to 22.5 cm in length and lacked ear plugs. While still used in some parts of Europe, the design was quickly superseded by binaural models. The first commercial stethoscope in 1829 featured a mahogany chestpiece and twin lead tubes, offering greater flexibility and comfort.
Throughout the 1840s–1850s, prototypes incorporating gum‑elastic tubing and aluminum chestpieces emerged. Marc‑Hector Landouzy introduced a gum‑elastic prototype in 1841, and Arthur Leared refined it in 1851. George Cammann’s 1852 design, with ivory or ebony earpieces, was regarded as the gold standard of the era. The 1859 differential stethoscope by Scott Alison introduced dual chestpieces, enabling triangulation of sound sources.
Electronic stethoscopes appeared in the 1890s, with Albert Abrams producing a functional model by 1902 that amplified cardiac sounds and differentiated between muscular and valvular activity.
Since the early 20th century, the basic binaural shape has remained stable, but materials have evolved. Plastic advances (polyvinyl chloride, Bakelite) and improved manufacturing have increased airtightness and flexibility, allowing mass production and widespread availability. Modern stethoscopes are typically assembled from metal and plastic components manufactured at separate facilities.
Raw Materials
A binaural stethoscope consists of earplugs, a binaural piece, flexible tubing, a stem, and a chestpiece. Earplugs are mounted on steel springs for a secure fit and are made from Delrin or silicone rubber. The binaural piece, stem, and chestpiece are forged from aluminum, chrome‑plated brass, or stainless steel. Flexible tubing is either polyvinyl chloride or latex. Dual‑diaphragm stethoscopes feature a steel ball‑bearing valve that switches between a flat and a cupped diaphragm. Anti‑chill rings, made of silicone or PVC, surround the diaphragm to improve suction and patient comfort.
The Manufacturing Process
Manufacturing is a multi‑site operation: metal parts and plastic components are produced separately, then assembled at a dedicated plant. High‑volume orders may include custom colors or hospital branding.
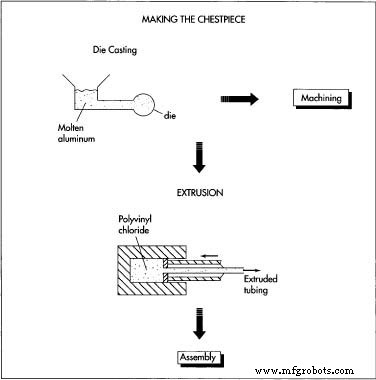
Making the Metal Chestpiece
- Aluminum is die‑cast and machined into the final shape. Stainless steel rods are lathe‑machined; brass is machined and electroplated. Binaural pieces receive threaded tops for earplugs and barbs at the base for tubing connection. Springs are attached and sealed.
Forming the Tubes
- Premium stethoscopes use “dipped” latex tubes, repeatedly immersed until the desired thickness is achieved. Lower‑cost models are molded or extruded. Tubing is attached by heating in warm water and then snugly wrapping over the barbs or by molding around the binaural piece.
Assembly
- Stethoscopes are hand‑assembled. The diaphragm is sealed in the chestpiece, anti‑chill rings are fitted around the rim, and earplugs are screwed on.
Packaging
- Economy models are shipped in sealed bags. Mid‑range units are boxed. Premium stethoscopes are packaged in sturdy boxes with die‑cut compartments, often in cases that hold 20–50 units for delivery to medical distributors or directly to hospitals.
Quality Control
Air leaks can reduce sound by 10–15 dB and allow ambient noise. Quality instruments meet tolerances of ~2.5 × 10⁴ mm to ensure airtightness. Manufacturers test each unit with pressurized air and tug tests. Visual inspections and acoustic reliability checks are performed at every stage.
Health‑care professionals receive extensive auscultation training, allowing them to differentiate normal from abnormal lung and heart sounds. Proper maintenance—regular inspection for leaks, cleaning with rubbing alcohol, and sterilization when required—preserves diagnostic accuracy.
For more detailed information, see the referenced figures:
Manufacturing process
- Amber: From Ancient Resin to Scientific Treasure – History, Properties, and Modern Uses
- The Guillotine: History, Design, and Legacy
- Silicon: Properties, Production, and Market Outlook
- The Ukulele: From Portuguese Roots to Modern Craftsmanship
- The Complete Guide to the U.S. Chicken Industry: History, Production, and Quality Control
- Compost: The Ultimate Soil Enrichment Solution
- Gelatin: From Ancient Protein to Modern Applications – Production, Uses, and Safety
- The Evolution and Manufacturing of Modern Pin‑Tumbler Locks
- Vodka: From Ancient Distillation to Modern Production
- Milk: Production, Processing, and Nutrition in the United States